PTSD MYTHS
Overview
Post-traumatic stress disorder (PTSD) is a mental health disorder. Many people believe things about mental health disorders that aren’t true. Here are some myths about PTSD.
Myth: PTSD is in your head. It does not exist.
PTSD does exist. It is a recognized mental health problem that has been studied for many years. You may get PTSD if you have lived through a traumatic event that caused you to fear for your life, see horrible things, and feel helpless. Strong emotions caused by the event create changes in the brain that may result in PTSD.
PTSD has not always had the same name. It also has been called combat fatigue or shell shock.
Myth: Only soldiers or people in war zones get PTSD.
Anyone who sees or goes through a traumatic event can develop PTSD. A traumatic event is a horrible and scary experience. During this type of event, you think that your life or others’ lives are in danger. You feel that you have no control over what is happening. These events include violent crimes, sexual assaults, childhood neglect or abuse, and natural disasters such as hurricanes or earthquakes. Your job also could expose you to traumatic events. First responders at a traumatic event, such as firefighters and police, can develop PTSD.
Myth: You should be able to move on after a traumatic event.
The strong emotions you may feel during the traumatic event can create changes in your brain that result in PTSD. You may not be able to “move on” because of this. It’s important to remember that PTSD is a medical condition. People with other health conditions, such as cancer, deal with the condition as best they can. The same is true for PTSD.
Myth: PTSD always happens right after the traumatic event.
PTSD symptoms can develop at any time after a traumatic event. Your symptoms may start soon after the event, or you may not have them until months or years later. They may come and go over many years.
Myth: People with PTSD cannot function.
PTSD can cause severe symptoms, but counseling, medicines, and support all help people adjust. People with PTSD have jobs and relationships. They enjoy life and are active members of their communities.
To view this article on Healthwise, click here
©1997–2019, Healthwise, Incorporated
 There’s nothing quite like a good comeback. It’s a testament to the determination of the human spirit, and a reminder of why second chances can be a great thing. The beauty of a comeback is that it happens in many forms. It could be an athlete getting back on the field after a major injury, or a determined older student going back to school to finally earn their degree. For Adam McCullough, it’s finding his way back into the driver’s seat.
There’s nothing quite like a good comeback. It’s a testament to the determination of the human spirit, and a reminder of why second chances can be a great thing. The beauty of a comeback is that it happens in many forms. It could be an athlete getting back on the field after a major injury, or a determined older student going back to school to finally earn their degree. For Adam McCullough, it’s finding his way back into the driver’s seat.
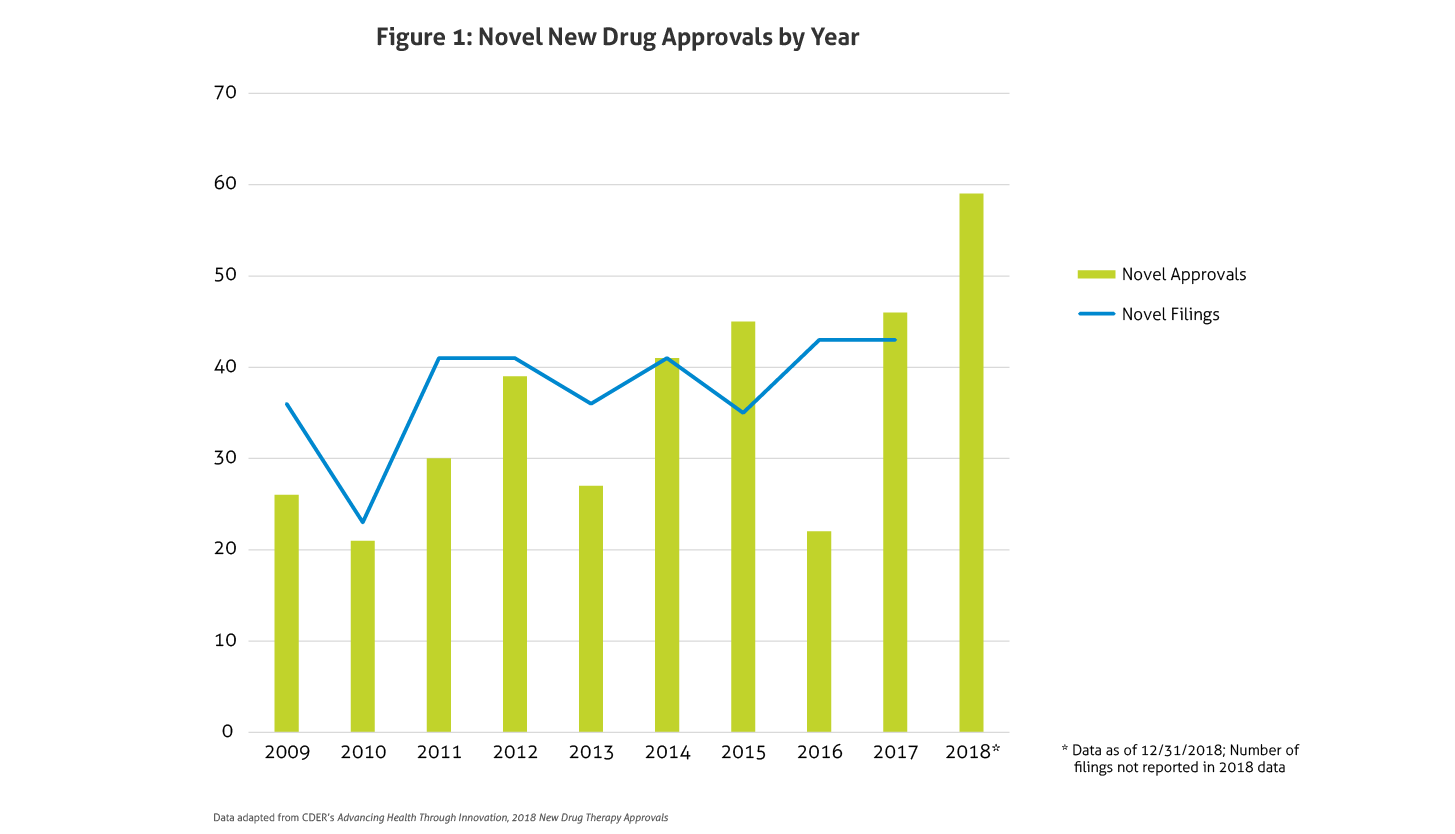
 Some of the notable 2018 approvals included the first non-opioid drug approved to reduce opioid withdrawal symptoms, a new antiretroviral for multidrug resistant human immunodeficiency virus-1, a new class of drugs for migraine (calcitonin gene-related peptide receptor antagonists), the first FDA-approved drug derived from marijuana, the first treatment approved for multiple sclerosis in children, expanded options for cystic fibrosis, and the first antibiotic approved under the Limited Population Pathway for Antibacterial and Antifungal Drugs.
Some of the notable 2018 approvals included the first non-opioid drug approved to reduce opioid withdrawal symptoms, a new antiretroviral for multidrug resistant human immunodeficiency virus-1, a new class of drugs for migraine (calcitonin gene-related peptide receptor antagonists), the first FDA-approved drug derived from marijuana, the first treatment approved for multiple sclerosis in children, expanded options for cystic fibrosis, and the first antibiotic approved under the Limited Population Pathway for Antibacterial and Antifungal Drugs.