Magellan in the News: Barry Smith Featured in Behavioral Healthcare Executive
|
Magellan’s own Chairman and CEO, Barry M. Smith, was recently featured in Behavioral Healthcare Executive, talking about the importance of prioritizing behavioral health as a part of disaster recovery.
In the article, Barry discusses how delivering innovative access to behavioral health services is critical to enabling not only physical, but emotional renewal.
A Strengths-Based Approach: How High Fidelity Wraparound Changed a Foster Family’s Path
|
Being a parent is one of the most challenging and rewarding jobs an individual can hold. When behavioral health challenges are added, it becomes even more difficult. Try, for a moment, to imagine being a foster parent to a child with behavioral health challenges. Where does one even begin to find the help and services they need to best care for their child?
Through our collaboration with the Wyoming Department of Health, Division of Healthcare Financing (Medicaid), Magellan in Wyoming coordinates care, including behavioral health interventions with other youth serving agencies in our system, using the High Fidelity Wraparound (HFWA) model to build a team of support for the successful management of complex conditions and behaviors in home- and community- based settings. The team creates steps to help youth stay in their homes, schools and communities. Through the 10 guiding principles of the program, families and youth have a voice in their care and choice in the kind of care they receive. We help to strengthen community support, understanding, and education of at risk youth ages 4-20 with complex behavioral health needs.
Magellan in Wyoming recently had the opportunity to hear from a former foster parent and HFWA graduate to discuss how the program benefited them through their challenges and supported their growth. “Opening my heart up to love and attachment with these children, parenting them with unconditional love, all the while knowing, they might not stay was difficult,” said the foster parent.
The siblings involved and their foster family cycled through numerous foster care workers in three years, creating more trauma for everyone. There was no stability and no consistency. Dealing with several different mental health diagnoses and many weekly appointments, in addition to the strain of everyday life, took a toll.
When this family discovered HFWA, they were naturally a little skeptical. They had experienced enough “new” things; however, this was the beginning of a completely new outlook on life. From the very start, HFWA taught the foster parent that it was okay to take a breath, to sleep and to ask for support. More importantly, it became evident that people wanted to help and be on the family’s team to help support them.
The family had spent so much time triaging the risk aspects of their children’s lives, that it had drained them of most of their hope. Through the strengths-based principles of the HFWA program, the family was able to gain new insight into ways they could focus on the local supports available to help them.
The program taught them to see the progress. By forming a HFWA team around the foster children and the whole family, they were able to gain some positive, strengths-based perspective along with stability and consistency.
HFWA empowered the family to have a voice and to use it effectively. “I knew all the people on my team before HFWA, but the program taught me how to use my voice. It taught me how to say what was going on and who to say it to,” said the foster parent. It was because of the family’s team, as well as community investment in the program, that today, the family is enjoying a life full of hope and possibility.
Care alongside Care: Treating Comorbid Medical and Behavioral Conditions
|
It’s 11:30 on a Tuesday night in the emergency department of a local county hospital. The doctor pulls back the curtain on his next patient and frowns. He has seen this man before. He looks down at the chart and recognizes the name. He’d been in about eight weeks before with trouble breathing and chest pains. Gears click in doctor’s memory, as he recalls this patient. His medical work-up had shown nothing acutely wrong. He’d been encouraged to take his usual medications, and sent home with instructions to see his regular doctor as soon as possible to make sure his chronic diabetes and congestive heart failure were under good control.
The doctor pulls a stool across the floor and sits down bedside.
“Hi Brian, what seems to be the trouble?”
“My chest. I couldn’t breathe. And I can’t seem to concentrate. I just don’t want to do anything.” Brian’s voice is listless and low, and he looks fatigued.
“I see you were in a couple of months ago. Did you go and see your regular physician?”
Brian shrugs but doesn’t say anything. His eyes are fixed firmly on the floor.
The doctor pauses. He looks at Brian for a while. The man looks like he hasn’t taken care of himself. His clothes are wrinkled, and he’s lost some weight since his last visit to the emergency department. The doctor looks over Brian’s vitals and labs. He finds nothing concerning on physical exam. He asks, “Brian, has anyone ever talked to you about depression?”
In the case above, Brian is a fictional character, but the situation is not. The co-occurrence of mental health disorders with physical ailments is common. A Substance Abuse and Mental Health Services Administration (SAMHSA) report found that 68 percent of adults with mental disorders have medical conditions, and 29 percent of adults with medical conditions have mental disorders. The most common of these is depression. Many research studies have found high rates of comorbid depression with chronic and terminal medical conditions. In many cases, the medical conditions or treatments for the conditions can cause depression. In others, the depression itself can lead to health behaviors that cause or worsen medical illness, and even higher risk of death. For instance, persons with depression have higher rates of smoking cigarettes than the general public. This can lead to heart disease. But, depression itself can also cause changes in brain chemistry and platelets, which can worsen existing heart disease.
Common Conditions with Comorbid Depression
Comorbid depression in some medical conditions is common. According to the National Institute of Health, there is a close relationship between depression and other physical ailments:
Alzheimer’s disease and other dementias
Cancer
Coronary artery disease
Congestive heart failure
Diabetes
Epilepsy
HIV/AIDS
Multiple sclerosis
Parkinson’s disease
Rheumatoid arthritis
Stroke
Systemic lupus erythematosus
Depression also has a negative effect on treatment and outcomes for these diseases. A 2015 published research study showed those with comorbid depression had more negative outcomes for their primary ailment than those who only had the primary ailment. Research also shows a lower quality of life, lower compliance with medical treatments, and lower rates of exercise and healthy eating habits for patients with comorbid depression compared to those with the same physical ailment(s) who did not suffer from depression.
This comorbidity has consequences beyond the health of the patient. People with multiple medical conditions are a rapidly growing and extremely costly segment of the US population. Patients with behavioral health disorders spend more on treatment for general medical conditions. When compared to those without depression, overall health care spending for medical conditions is higher than those without, in addition to treatment for the depression itself.
Improving Care for Comorbid Behavioral Health Conditions
The first step is identifying patients with comorbid behavioral health conditions before they reach the dangerous and costly levels discussed above. The primary care setting may be the best place to first find depression. But how?
Magellan’s Screen and Engage program is an innovative, user-friendly application that primary care physicians (PCPs) can use to identify patients at risk for a mental illness. Using a Magellan-provided iPad, the patient answers questions about his or her health and well-being while waiting for an appointment. The screening tools are also available in Magellan’s Virtual Care Solutions. Magellan’s proprietary algorithms assess the results, identify potential behavioral health issues and suggest recommendations for treatment, and flag clinicians to engage the patients.
The benefits of the tool are clear. Given the limited amount of time that a PCP has for each appointment, he or she must focus the conversation on the primary reason for the visit. As such, there is little opportunity to probe for behavioral health concerns. By conducting the screening before the short appointment, the PCP has a chance to be notified of the screening results, and discuss them during the visit.
Screening for behavioral health conditions is just the first step. Step two is treating them. In general, depression is treated with either medications and/or cognitive behavioral (CBT) psychotherapy. CBT is a specific type of therapy that relies on identifying and changing ones thoughts that can lead to depression. Research shows that the combination of the two is better than either done separately. While it may be easy to receive anti-depressants from medical doctors, it is often difficult to find CBT.
Cobalt, Magellan’s computerized Cognitive Behavioral Therapy (CCBT) program, is a cost-effective solution to address common behavioral health conditions. Cobalt provides CCBT online or through a smartphone/tablet app. This makes face-to-face CBT—proven to work but often difficult to find providers, especially in rural areas and for working people—available anywhere, any time. It is also a more private approach to CBT. Patients can access treatment from their homes versus an office.
Computerized CBT has proven to be just as effective as in-person CBT. Magellan offers Cobalt modules for insomnia, depression, anxiety, substance use disorder and obsessive-compulsive disorder, treating more than 90 percent of behavioral health conditions seen in primary care and behavioral settings.
Tackling Comorbid Conditions for a Healthy Future
At Magellan, we have made it our mission to help individuals like Brian, whose case is all too common. Tackling comorbid behavioral health issues alongside common medical conditions is one way we do it. Investing in and using new technology, we can identify more people who need help and expand their access to effective, proven treatments.
What is HEDIS and What Does it Mean to You?
|
Magellan’s collection of HEDIS (Healthcare Effectiveness Data and Information Set) quality measures for 2017 has entered the final phase of data collection. You’ve probably heard of the acronym HEDIS – but what does it stand for and what does it mean to you? The Healthcare Effectiveness Data and Information Set – HEDIS — was created by the National Committee for Quality Assurance (NCQA) to measure the clinical quality performance of health plans. This is accomplished through the collection and analysis of data documenting the clinical care received by individual plan members from providers, influenced through activities and programs delivered by the health plans. The data is aggregated and reported collectively to reflect the ‘collective’ or population-based care received by the plan’s membership. These reports have become a major component of quality rating systems that measure the clinical quality performance of health plans by Centers for Medicare & Medicaid Services, states offering Medicaid and other entities. Right now, Magellan has entered the final phase of data collection for HEDIS quality measures for 2017.
There are 91 HEDIS 2017 measures, but it’s important to note that the number may vary from year to year as new measures are added to the set and some are retired. The measures cover many aspects of healthcare including preventive care such as screening tests (e.g., mammograms) and immunizations, management of physical and mental health conditions, access and availability of care, patient experience, utilization and relative resource use. Data is reported individually for each product and line of business
Measure data is collected is a variety of ways. Claims are the major source of data, but specific measures may also allow plans to survey members or to access member medical records for additional data not captured in claims. This type of data collection (combined claims and chart data) is called hybrid. The final phase of data collection for health plans choosing to do hybrid runs from January through May and is often called MRR for medical record retrieval, or simply ‘chart chase.’ Final HEDIS data covering services rendered in 2016 and prior will be submitted to NCQA by June 15, 2017. Final health plan ratings for all lines of business are published on the NCQA website by October 2017.
For health plans, HEDIS ratings can be very important. The scores on measures can help them understand quality of care being delivered to their members in some of the most common chronic and acute illnesses. Higher scores can help compete more effectively in various markets. HEDIS score reporting are often required in public markets as well, where the results are often reported to the states, or occasionally counties, in which the plans reside.
Behavioral health and pharmacy are well represented in the HEDIS measure set. Behavioral health has multiple measures that include ensuring continuity of care, appropriate psychotropic medication management/adherence, and initiation and engagement of drug and alcohol abuse treatment. Pharmacy measures focus on medication management of acute and chronic physical and mental illness, appropriate medications in the elderly, and management of polypharmacy. Specialty measures are directed toward inappropriate imaging.
So, what is the value of HEDIS to Magellan? Aside from being a collection and reporting contract requirement for many of our customers and our own health plan, HEDIS gives Magellan valuable information about the populations we serve.
By following the behavioral health data, we collect, for example, we can identify gaps in network performance in patient follow-up patterns, management of drug and alcohol abuse, and prescribing and adherence to medications. This allows us to design and implement interventions that can improve outcomes and reduce cost of care.
The same type of analysis/intervention applies to physical health conditions. Analysis of HEDIS data helps identify gaps in care, particularly preventive care, in such important and chronic populations as patients with diabetes mellitus, patients with cardiovascular disease, and patients with lung disease. We can also identify and address at-risk pediatric populations who fail to complete preventive care such as immunizations, dental and well-child care.
As the healthcare industry moves more and more toward value-based purchasing, all providers, insurers and their vendors are necessarily increasingly focused on the quality of care that is delivered. The impact of this should be better outcomes for our members.
See the impact of opioid addiction in this new infographic
|
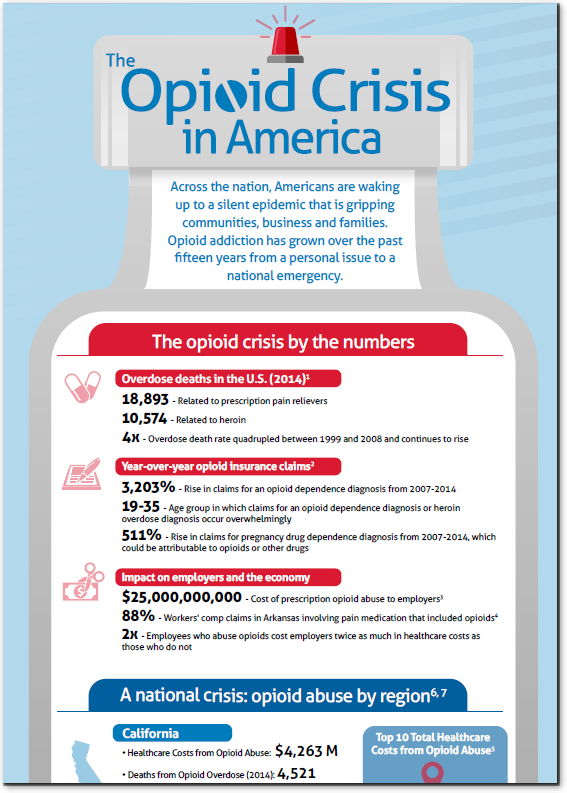
Opioid addiction has grown over the past fifteen years from a personal issue to a national emergency. A new infographic from Magellan Healthcare reveals the devastation that this epidemic is causing.
In 2014, there were 18,893 overdose deaths related to prescription pain relievers
There was a 3,203% rise insurance claims for opioid dependence diagnosis from 2007-2014
Prescription opioid abuse is costing employers $25,000,0000 a year
The opioid addiction crisis is causing such an unprecedented amount of harm precisely because it is such a complex, multi-faceted issue. Those looking for answers as to how such an epidemic could have happened, will need to examine a swath of individual problems, including:
The enormous quantity of prescription opiates
The limited patient knowledge of opiate risk
That diversion of opiates to family and friends is so common that only 20% of those with opioid abuse problems are actually using opioids prescribed to them
The struggle to adequately assess patient’s substance use history and risk of addiction when prescribing opiates
The lack of clear guidance as to who should receive opiates and for how long
The difficulty in maintaining patient adherence to withdrawal management treatment plans.
New solutions are needed to tackle each of these individual issues. At Magellan Health, we intend to do precisely that. The opioid addiction crisis has already taken a huge toll and it grows worse every day. It is manifesting itself in myriad ways among thousands of communities across the nation. At Magellan Health, we have an unyielding commitment to ending this epidemic.
 Magellan’s own Chairman and CEO, Barry M. Smith, was recently featured in Behavioral Healthcare Executive, talking about the importance of prioritizing behavioral health as a part of disaster recovery.
Magellan’s own Chairman and CEO, Barry M. Smith, was recently featured in Behavioral Healthcare Executive, talking about the importance of prioritizing behavioral health as a part of disaster recovery.