Going Beyond Traditional Benefits: Healthcare Systems Begin to Address Social Determinants of Health
Two patients, both 73-year-old males with newly diagnosed congestive heart failure, are seen by the same provider and prescribed the same therapeutic regimen. Despite the similarities, the 2 patients experienced drastically different therapeutic outcomes. These divergent outcomes were not attributable to the clinical care they received but instead to non-clinical factors surrounding each patient’s circumstances. These non-clinical factors are also referred to as social determinants of health (SDOH). According to the Centers for Disease Control and Prevention (CDC) website, SDOH are conditions in the places where people live, learn, work, and play that affect a wide range of health risks and outcomes. Some key SDOH that may influence clinical outcomes include housing insecurity, food insecurity, lack of transportation, and lack of family or other social support.
It is widely known that social and economic factors have significant impacts on health outcomes of both individuals and communities. At a population level, it has been estimated that clinical care accounts for only 20% of a community’s health outcomes while the remaining 80% is related to a combination of health behaviors (e.g., diet and exercise), the physical environment (e.g., housing security), and socioeconomic factors (e.g., education and social support). Despite this insight, addressing SDOH has traditionally been the purview of government and charitable organizations rather than healthcare providers. However, with the shift toward value-based reimbursement and increased accountability for the costs and health status of patients, there is an incentive for health plans and providers to further consider the social and economic barriers that contribute to poor health outcomes. Models are being developed that link healthcare systems, providers, and community resources in an integrated fashion to address SDOH. These models are evolving from systems that rely on acute episodes of care to a coordinated system focused on prevention and care management.
As the largest payer for healthcare in the United States, Medicare has also recently begun to make accommodations in order to address SDOH in the privately administered Medicare Advantage (MA) program. MA is a capitated system placing health plans that administer MA benefits at risk for the cost of caring for each beneficiary. MA plans are permitted to offer supplemental benefits beyond traditional Medicare offerings as long as those benefits are “primarily health-related.” Historically, the most common supplemental benefits offered by MA plans have been services not traditionally covered by medical insurance such as vision exams, hearing tests, and preventative dental services.
The Centers for Medicare & Medicaid Services (CMS) have recently begun to implement regulatory changes allowing MA plans more flexibility with regard to these supplemental benefits. First, the definition of “primarily health-related” has been expanded. Examples of this expanded interpretation include providing in-home support for activities of daily living (ADLs) or installation of grab bars in the bathroom in order to prevent injuries and reduce avoidable emergency room utilization. In addition, supplemental benefits that may reduce exacerbations of existing illnesses, such as installing air conditioning units or providing carpet shampooing for patients with asthma, may be considered. Beginning in 2020, MA plans may offer chronically ill patients additional benefits that directly impact SDOH, such as expanded meal delivery options to address food insecurity and transportation for non-medical needs like grocery shopping. In announcing the expanded options for MA plans, CMS Administrator Seema Verma said the changes “give plans the ability to be innovative” and the changes permit “benefits and services that address SDOH for people with chronic disease.”
The shifts occurring in healthcare delivery, including the expansion of accountable care organizations (ACOs), the rise of capitated reimbursements, and penalties associated with hospital readmissions, incentivize healthcare systems to become increasingly focused on holistic care for beneficiaries. By addressing individual and population SDOH, healthcare systems, providers, and community support can be integrated to improve health outcomes and reduce unnecessary healthcare utilization.
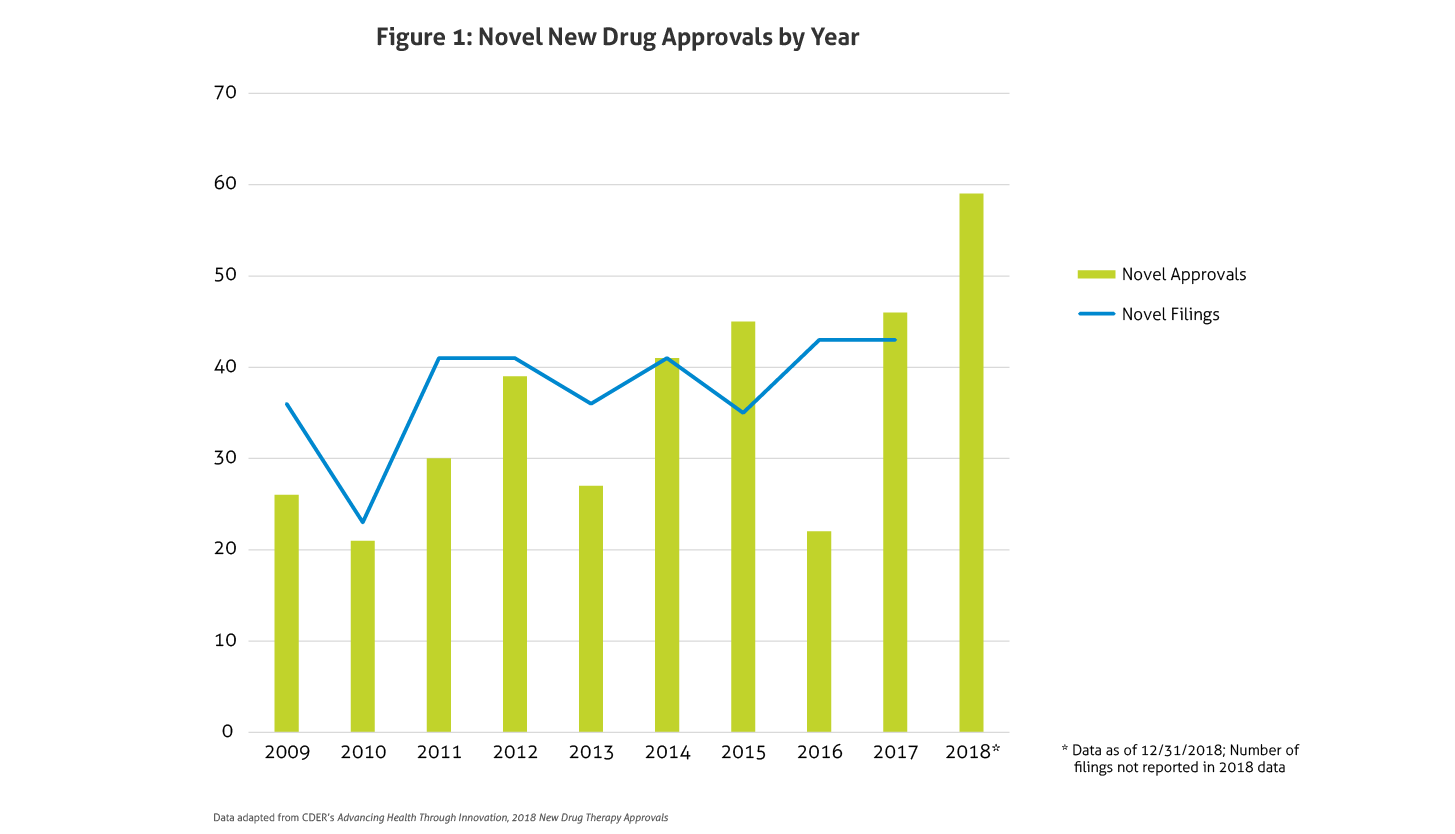
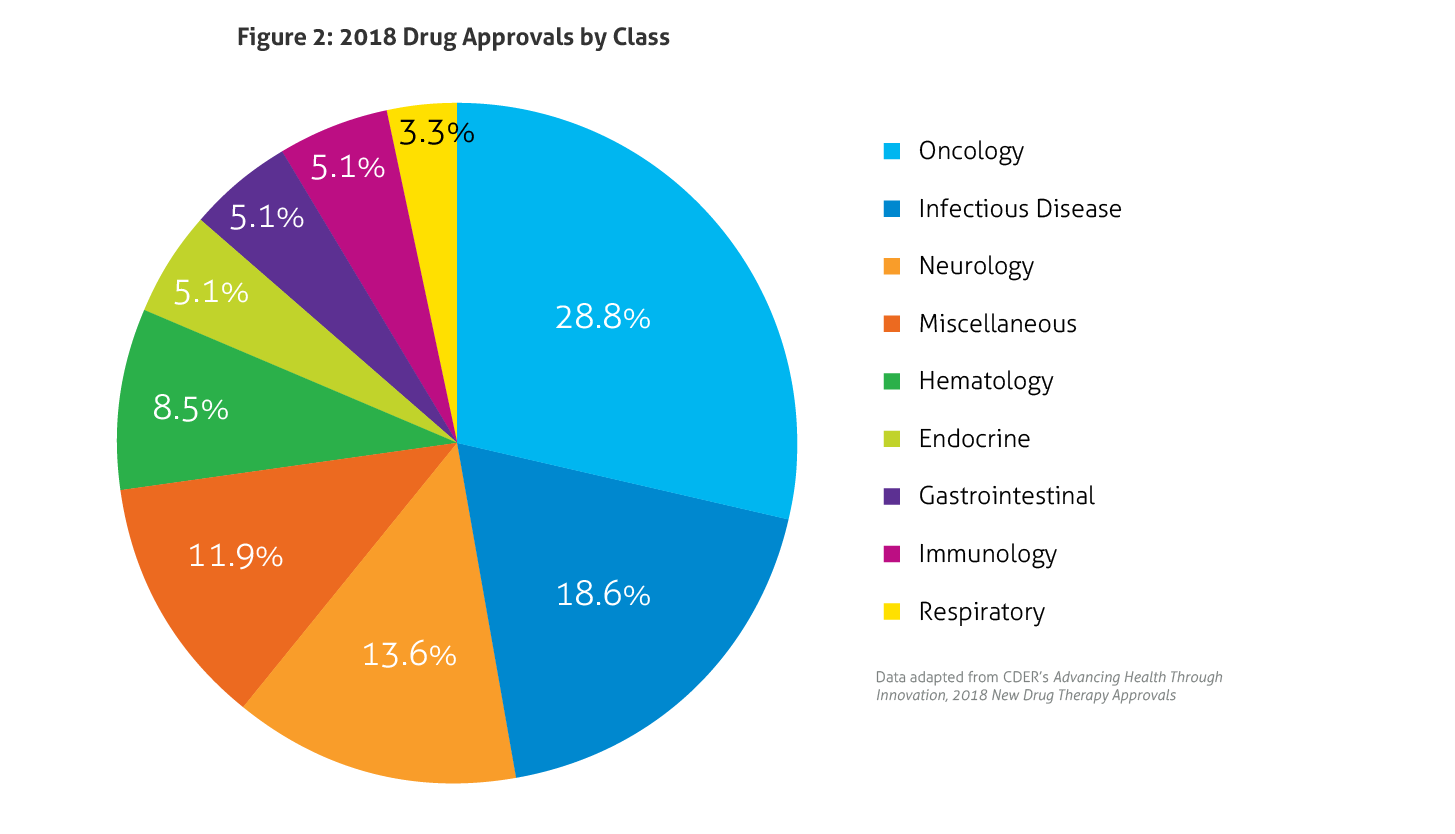 Some of the notable 2018 approvals included the first non-opioid drug approved to reduce opioid withdrawal symptoms, a new antiretroviral for multidrug resistant human immunodeficiency virus-1, a new class of drugs for migraine (calcitonin gene-related peptide receptor antagonists), the first FDA-approved drug derived from marijuana, the first treatment approved for multiple sclerosis in children, expanded options for cystic fibrosis, and the first antibiotic approved under the Limited Population Pathway for Antibacterial and Antifungal Drugs.
Some of the notable 2018 approvals included the first non-opioid drug approved to reduce opioid withdrawal symptoms, a new antiretroviral for multidrug resistant human immunodeficiency virus-1, a new class of drugs for migraine (calcitonin gene-related peptide receptor antagonists), the first FDA-approved drug derived from marijuana, the first treatment approved for multiple sclerosis in children, expanded options for cystic fibrosis, and the first antibiotic approved under the Limited Population Pathway for Antibacterial and Antifungal Drugs.