Reasons to tell people about it
Whether or not you discuss your condition with family, friends or coworkers is a personal decision. You may find it hard to talk about your diagnosis, or you may be concerned about how others will react. Ideally, the people around you will accept your illness and be encouraging. Bear in mind that they might not know very much about your condition. While they may want to help you, they may not know the best way to help. You can give them a better chance to support you by thinking ahead about how to tell them about your mental illness.
Why to tell
One reason to tell others about your mental illness is to receive encouragement. Talking to a sympathetic friend or loved one can reduce your stress level and improve your mood. You may no longer feel like you are keeping a secret. You may also want to ask for concrete support, like help finding treatment or rides to appointments. Or, maybe you want to share your crisis plan with a trusted family member.
When to tell
Telling people is a very personal decision and should only be done when you’re ready. It might help to practice how you tell people with a professional, such as a therapist. You can discuss your worries and how to react to issues, questions and comments that might arise. Practicing may help you clarify how you feel about your condition and inform who you want to tell.
Make sure you are in a calm environment when you introduce the topic and give the person time to adjust to the idea, especially if he or she don’t know a lot about your condition.
If you are compelled to tell people during a period where you are unwell, try to locate the most supportive person in your life for support as you go through the process.
Who to tell
You are the expert on your condition and can decide for yourself the right or wrong number of people to tell. Some people will benefit from telling many family and friends. Others may benefit by telling a couple of close friends and waiting to tell others.
Make a list of the people you’re considering telling and include those closest to you. Also list the most emotionally skilled people you know, even if you don’t know them that well.
Personal relationships
When telling family, friends or someone you are in a romantic relationship with about your condition, their response will generally go in one of three directions:
- The person is genuinely comfortable with your disclosure and things stay the same
- The person is very uncomfortable and ends or changes the relationship
- The person says he or she is fine with it, and then does a fast or slow fade from your life
Coworkers
In a job, you have to weigh the advantages against the disadvantages of being open. Weigh the potential negative impact on things like stigma from coworkers against your need for special accommodations, which are considered part of your civil rights. Before you share information about your condition, you should learn about your legal rights and also take into consideration your work environment. Consider approaching your Human Resources contact to gather support.
Once you’ve told someone, you’ll understandably be concerned about their reaction. One sign they can handle it is if they treat you the same during or after the disclosure. Friends stay friends. Colleagues stay polite and interested. If you continue to get the same “vibes” from people, you can be pretty sure that your disclosure has not changed the relationship for worse. And that is the best outcome of all.
Knowing that certain people are aware of an important part of your life and that they accept you and support you can be incredibly helpful and liberating. While some people may disappear, it’s better to have strong social supports around you.
Being able to offer emotional support is not something that everyone knows how to do. It’s a skill that takes practice. Some people may not be able to offer emotional support. If you have relatives or friends who lack this skill, that doesn’t mean they don’t love you. Most likely they don’t understand or fear they may say the wrong thing.
Remember that some conditions may cause you to not want to reach out for help. Sometimes the help from others is exactly what is needed to move toward recovery.
What to talk about
You can get the best support possible by planning the conversation. Consider including three items:
- “Process” talk
- Specific problem
- Suggestions for how loved ones can help
“Process” talk means “talking about talking,” rather than talking to share information. Prepare your listener for an important conversation by using “process” talk. Here are some ways to begin a process talk:
- “I want to talk to you about something important. I’m not sure how to talk about it, though. Can you just listen to me and try to understand? I’m hoping I’ll feel better after talking about it with someone, but I need you to be patient.”
- “There’s something going on in my life that’s bothering me. I think I need to talk to someone about it. I feel embarrassed about it, though, so please don’t laugh it off or make a joke out of it.”
- “I’m not sure if this will make sense. I feel uncomfortable talking about it, but I want to tell someone.
Concrete examples of what you mean by “mental illness.” Every case of mental illness is different. To get the best support possible, share one or two examples of what’s causing you stress:
- “I think something’s wrong because I can’t sleep more than a couple hours at night. It’s hurting my work and I feel out of control.”
- “I’ve started skipping classes sometimes. I’m worried I’ll stop leaving the apartment if I don’t get help.”
- “The doctor said I have bipolar disorder. Sometimes I feel like things are getting out of control and I’m not sure how to keep myself together.”
Suggest ways to support you. Family and friends may not know what they can do to help. You can get the best support by asking for specific types of help:
- “I’m scared to make an appointment because that’s like admitting there’s something wrong. But I need to see a doctor. Can you help me find one and follow through?”
- “I’m not thinking clearly these days. I’m getting treatment for a mental illness, but it might take a while to feel right. Until then, when I do something that makes you uncomfortable, can you please tell me what I’m doing instead of getting freaked out?”
- “I’m not supposed to drink alcohol with my medications. I’m going to try not to drink at parties, but I need my close friends to encourage me and help me keep my social life.”
- “I’m feeling better. But once in a while, can you tell me you’re there for me and give me a hug?”
- By telling the right people and suggesting ways for loved ones to help, you can start building a strong social support network. At first, you might be afraid to talk about your experiences. But don’t give up looking for support and encouragement from others. You’ll discover that many people want to help you.
You don’t have to share everything. Decide in advance what parts of your experience you’ll talk about and what parts you won’t. Stand by your decision. It’s perfectly understandable to answer a question with a statement like “I’d rather not talk about that right now.”
Keep in mind
Share the good things. Explain how your illness has taught you new things, or about experiences you were able to have in spite or, or because of, your illness.
Set boundaries. Be clear with people about when you want their advice and when you just want them to listen. Also realize that people come with their own opinions, informed and otherwise, so be patient when explaining. If they try to discredit you, gently remind them that you are the one living with the illness, and you know yourself best.
Let them know how they can support you. Everyone has different needs, and different people respond in different ways. Think about your needs ahead of time, and about whether this person can support you, if there are resources that would help her or him understand what you’re going through, or if she or he says no. Some people may not be able to handle disclosure, so it may be difficult to expect support from them. There are many people who will probably feel honored that you shared this with them, and whom will be happy to do what they can.
Help is available. For additional information, visit MagellanHealth.com/MYMH
Source: NAMI
This document is for your information only. It is not meant to give medical advice. It should not be used to replace a visit with a provider. Magellan Health does not endorse other resources that may be mentioned here.
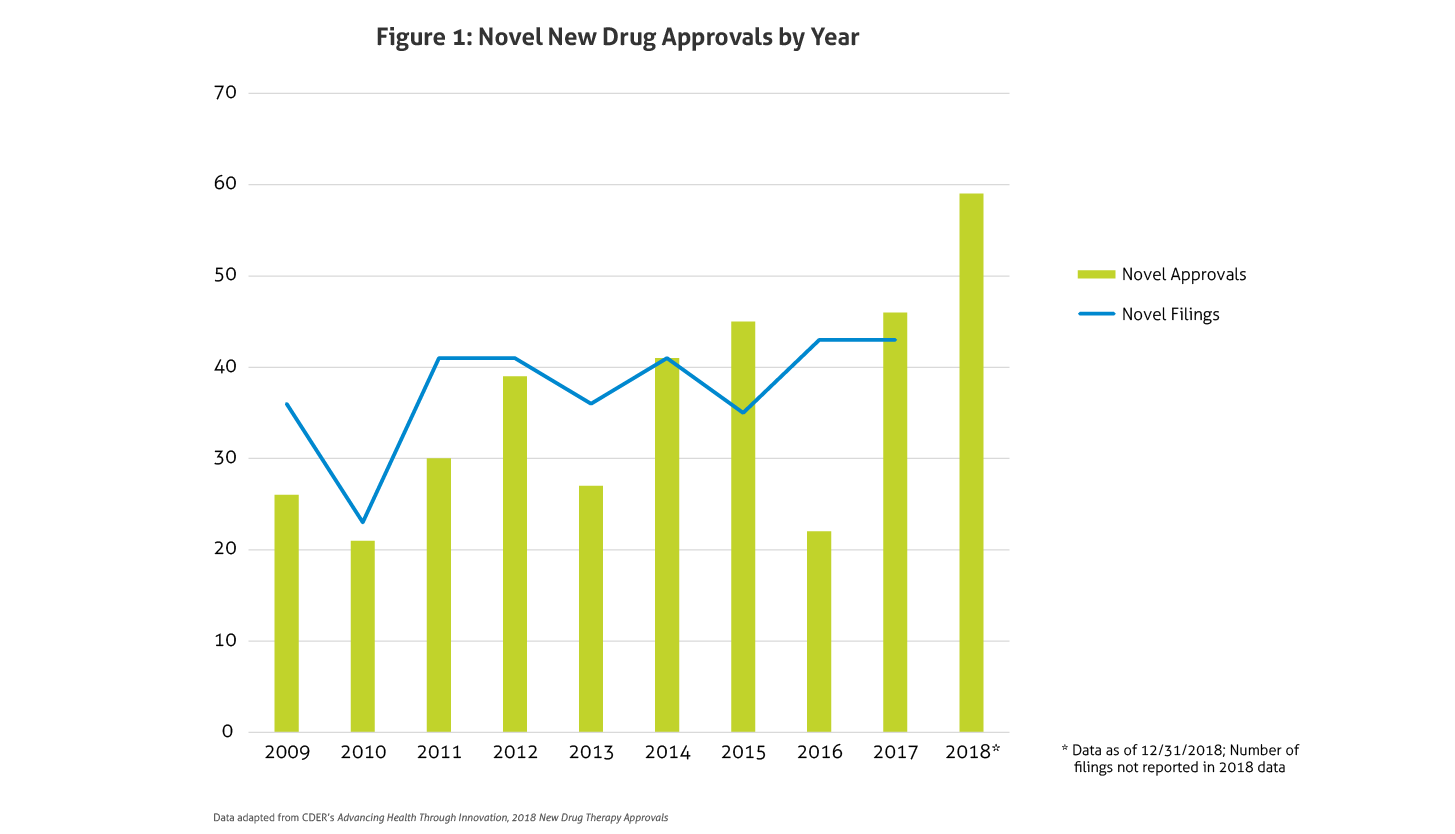
 Some of the notable 2018 approvals included the first non-opioid drug approved to reduce opioid withdrawal symptoms, a new antiretroviral for multidrug resistant human immunodeficiency virus-1, a new class of drugs for migraine (calcitonin gene-related peptide receptor antagonists), the first FDA-approved drug derived from marijuana, the first treatment approved for multiple sclerosis in children, expanded options for cystic fibrosis, and the first antibiotic approved under the Limited Population Pathway for Antibacterial and Antifungal Drugs.
Some of the notable 2018 approvals included the first non-opioid drug approved to reduce opioid withdrawal symptoms, a new antiretroviral for multidrug resistant human immunodeficiency virus-1, a new class of drugs for migraine (calcitonin gene-related peptide receptor antagonists), the first FDA-approved drug derived from marijuana, the first treatment approved for multiple sclerosis in children, expanded options for cystic fibrosis, and the first antibiotic approved under the Limited Population Pathway for Antibacterial and Antifungal Drugs.